Why are only some of us living longer?

Our Senior Evidence Manager examines the shocking health inequalities present in the UK today – and how we should tackle them.
There are staggering differences in health and life expectancy, which are strongly influenced by wealth and race. We explore what’s behind the shocking disparity.
In February 2022, in the wake of the COVID-19 pandemic, the government launched an independent review of health inequalities in the UK, the findings of which are expected to be published in a White Paper later this year.
These health inequalities are truly shocking.
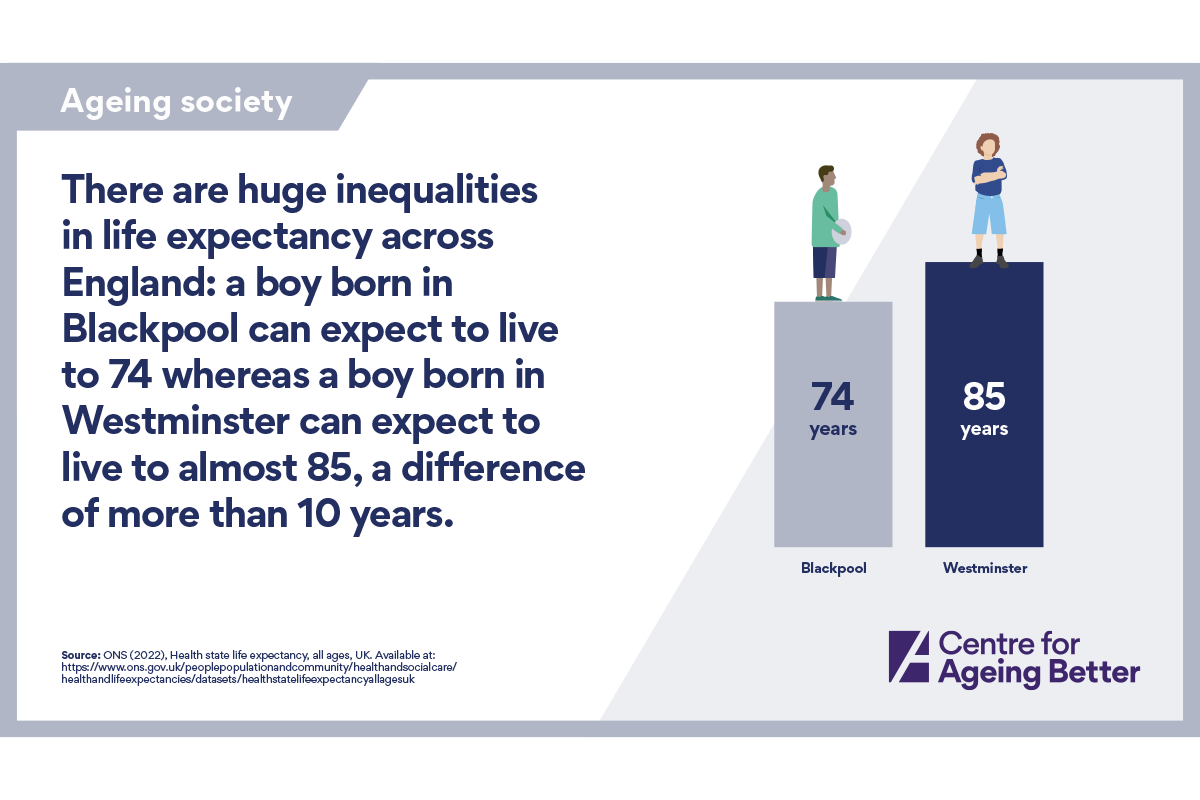
As shown in our updated Living longer infographics that we’ve published today, a boy born in 2022 in Blackpool can expect to live to 74 while one born in Westminster can expect to live to almost 85.
People living in the wealthiest areas have almost twice as many years disability-free ahead of them at age 65 (12 years) as those in the poorest (six years). Recent analysis by the Health Foundation has shown that, on average, a 60-year-old woman in the poorest area of England has levels of diagnosed illness equivalent to that of a 76-year-old woman in the wealthiest area. And the rate of poor health of Bangladeshi women in their forties is equivalent to that of White British women in their seventies.
Urgent action is needed to improve the nation’s health and narrow the gap between the poorest and the wealthiest, and between people from ethnic minority backgrounds and the White majority.
One important strategy – and one we would expect to see reflected in the White Paper – is a shift in focus away from acute and crisis care towards prevention. Our work on active travel stemmed from the understanding that keeping physically active helps to delay the onset and progression of many age-related health conditions and plays an important role in helping to manage the impact of health conditions once we develop them. We're therefore delighted at the news that doctors will prescribe walking and cycling to boost physical and mental health and ease the burden on our NHS.
But, while welcome, a preventive approach to health will not be enough. Instead, the White Paper must explicitly acknowledge the social determinants of health; these are, in the words of the World Health Organisation, “the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.”
Incredibly, the role played by the conditions of daily life was recognised as long ago as 1848 by the German physician Rudolf Carl Virchow, who, while reporting on a typhus epidemic in Upper Silesia in 1848, wrote “Medicine has imperceptibly led us into the social field and placed us in a position of confronting directly the great problems of our time.”
If proof were needed that we cannot fix health inequalities without looking at the wider conditions of our lives, then consider this: medical care has been found to account for just 10–20% of people’s health outcomes with the many social determinants of health responsible for the remainder (that is, 80-90% of a person’s health status). Moreover, according to Professor Michael Marmot, the higher the inequality in health in a country, the poorer the health of the population as a whole. So fixing inequality benefits all of us.
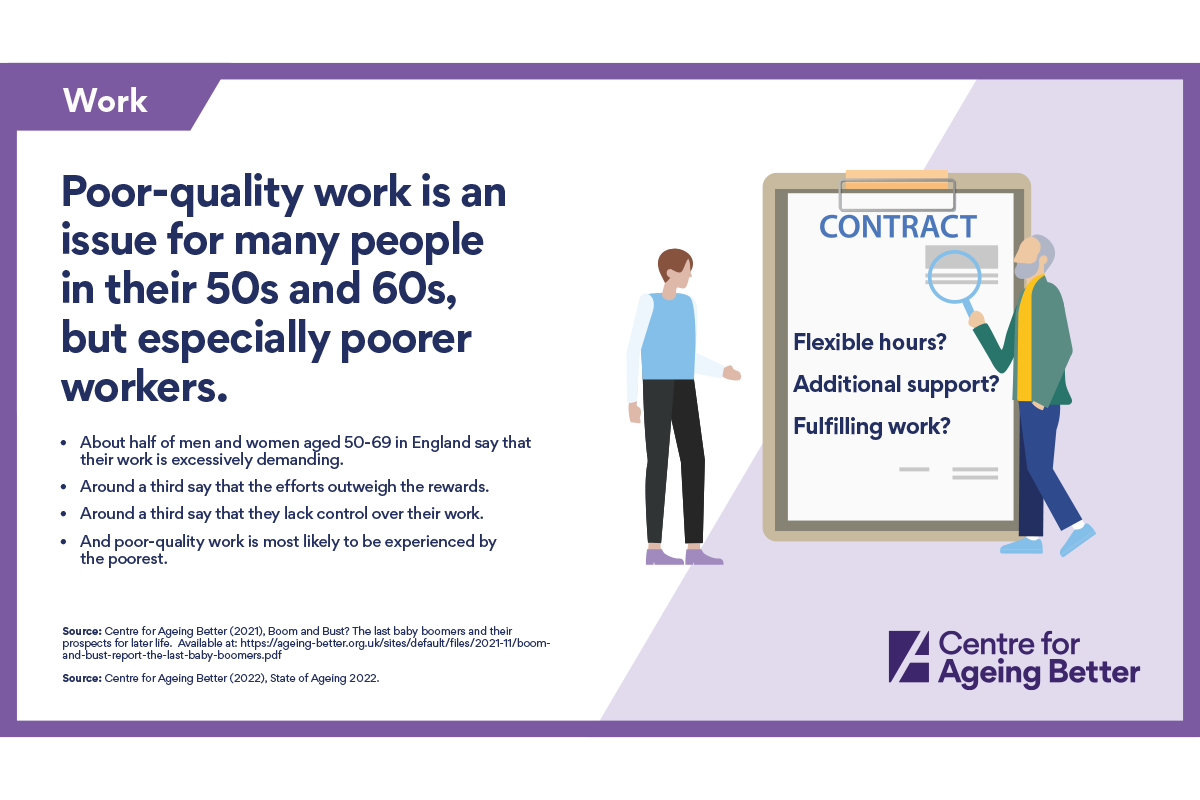
The breadth of the factors that shape a person’s health and wellbeing in later life are reflected in our updated 'Living longer' infographics. These cover the state of our homes, employment, finances and connections in our communities – and all of these can impact our health. Consider for example the role of poor-quality work. According to research by the Health Foundation, the proportion of employees in poor-quality work who report poor health is twice as high as for employees with no negative job aspects. And as the infographic shows, poor-quality work is particularly an issue for poorer workers.
It should be abundantly clear then that the forthcoming White Paper on health disparities must go further than a narrow focus on health care and prevention. After all, the government’s own Office for Health Improvement and Disparities provides a Wider Determinants of Health tool “designed to draw attention to the broad range of individual, social and environmental factors which influence our health and provide the public health system with intelligence on the wider determinants of health to help improve population health and reduce health inequalities”.
We echo the NHS Confederation in its call for the White Paper to require health equity in all policies and that “all government departments consider (and justify) the differential mental and physical health impacts of their policies”. In short, the White Paper must be directed at the whole of government and not just the Department for Health and Social Care.
Only then can we have any change of tackling the obscene and growing health inequalities in this country today.

